Okay I think it's about time I start making a series of posts on dental sleep medicine. I have been doing Derek Mahony's mini residency for almost a year now and have learned a lot. What this series will cover: -Pathophysiology of OSA, snoring ,TMD and bruxism -The link between Bruxism, TMD and OSA -Parasomnias -Clinical examination -Sleep studies -Management strategies -Side effects of treatment and their management
Posts
Getting a good contact with large GICs

Today I was in a situation where there was a 46 tooth with an MODB fracture. The mesial and distal margins were equigingval. The tooth is set for an endo or and exo but I did not have the required equipment to perform either (In the dental truck). So the plan is a temporary restoration and the patient will seek treatment privately. There are two options from here. -Restore to decent contour and contact -Restore with a stump with open contacts Ideally I would have a good contact to stop food packing but at a copmromise I would consider a wide open contact to allow interdental brushes to fit in. Without anaesthesia which was my plan, Wedges would be painful and making a contact would be difficult. This was due to the equigingival margin. In the past to make a decent contact I have used a light cure GIC like Fuji2LC and restored in stages. Sectional matricies are usually too unstable to be used due to the minimal surface area they are in contact with the tooth and there is the same ...
Placing anterior matrix strips
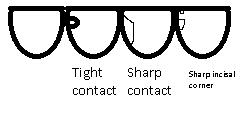
In the past I have had difficulties in placing the clear mylar strips in class 3 cavities where there is a strong or a sharp contact as in the picture below. -Tight contacts tend to bunch up the matrix and when you eventually jam it down it has a poor contour -Sharp contact will do the same, where there is a thin bit or supported incisal edge and it will catch or dent the matrix -Sharp incisal corner i.e if there is a small chip just off the location of the incisal corner. This may be in composite veneer cases where you want a clear strip to separate the teeth or in class 3 cases in a bruxer. I have found the matrix may want to go into this little divot rather than sliding between the teeth Solutions are currently: -Take a bur or polishing disc and cut off the obstruction. This is destructive especially for the tight contact case where there is a fair bit of supporting tooth structure -Use a tofflemire matrix or other metal matrix. This is more rigid and can be forced between th...
Handling GIC
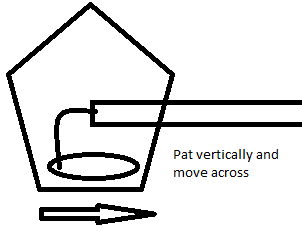
One issue with material handling I have had in the past is with GIC. Something about the texture and the fact that it self sets makes it incredibly difficult to handle in my hands. Occlusal cavities aren't too bad as you just bog it up making sure to avoid incorporating air bubbles and then trim down the rest but in the aesthetic zone I do find it difficult to place and polish to an acceptable result. Some strategies I've used in the past: -Bond on a microbrush or instrument to improve handling -Bog up and trim back: Tended to have a poor result with bur marks in the GIC -Cover with bond and cure for a good finish: Apparently G coat plus is used for this which I haven't had experience with yet Currently my strategy during class V GIC placement is to overfill the cavity just very slightly (practice makes perfect) then to use a flat plastic or a carver to pat the material down and adapt the margins. I find patting works better than spreading as he material tends to pu...
Some rubber dam tips
Hi, just some tips for placing rubber dam that come to mind. Not sure if this is a repeat from the past. Rubber dam is the best and most reliable way to isolate teeth. I do believe that it will improve outcomes of any treatment it is used in. It is essential in endodontics. Imagine a sharp endo probe or caustic sodium hypochlorite going down the patient's throat. Ouch. -I have been using No 7 Hygienic clamps for molars, 2A clamps for premolars, anterior clamps for anteriors. This seems to fit most purposes. -Do be cautious of clamps on heavily broken down or root filled teeth. There is a lot of force from those prongs -When you are applying topical to the injection site, place some on the gingiva around where the clamp will go. it will make it much easier to tolerate the clamp -You can apply the remaining topical to the underside of the dam in the interproximal area as a lubricant to slide down between the contacts -This video pretty much shows how I use floss ligatures htt...