Dawson's Occlusion: The design of the masticatory system
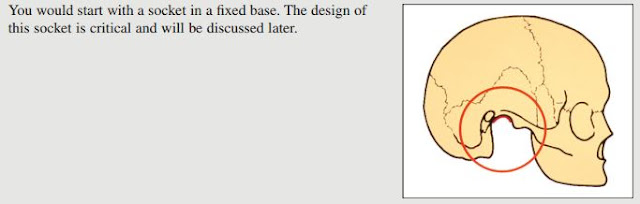
The goal for all occlusal therapy is a peaceful neuromusculature. If there is any loss of equilibrium, the muscle will try to regain equilibrium. In a war between teeth and muscle, the teeth will lose. This manifests as tooth wear, mobility, fracture and movement. It is essential to understand the role of the TMJs in occlusal design. As clinicians we must ensure that the TMJ in a reproducible and physiologic position (Centric relation) before the occlusion can be properly assessed and treated. Dawson explains the importance of occlusal harmony by taking a mechanical perspective on the design of the masticatory system. In the design of the teeth, it is important to note that the Jaws and TMJ developed before the occlusion therefore, the occlusion must fit into the preestablished maxillomandibular relationship.Correct phyisologic jaw position must therefore be determined before we can determine the correct alignment and occlusal relationship of the teeth. Th...