Pulpitis analogy
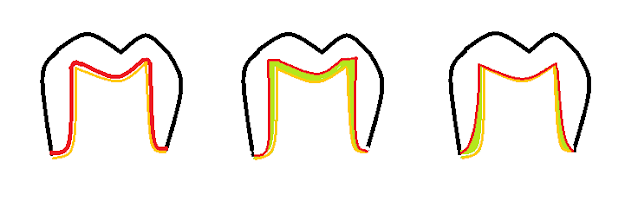
I thought of a good analogy as to why pulpitis pain can be so severe for our patients. I don't know how useful this will be in a clinical scenario but it may come in handy in the future. Have you ever put a ring on that was too tight and you were scared because you knew that if you couldn't get it off at first then it would be harder and harder to get off? The problem is that as the finger is irritated and compressed, the blood flow increases to the area and the soft tissue swells. On top of that, The ring is a hard material and doesn't expand in response to the swelling tissue. The same is true in a tooth. The tooth is the proverbial ring and the pulp tissue is the finger. Localised insults cause an increase in blood flow to the area due to the inflammatory cascade but the pulp is entombed in the tooth and there is nowhere for the excess pressure to go and this increase in pressure causes firing of nerve endings that manifest as pain. If we burn our skin, the skin swells,...