Anterior aesthetics part 4: Anterior tooth forms

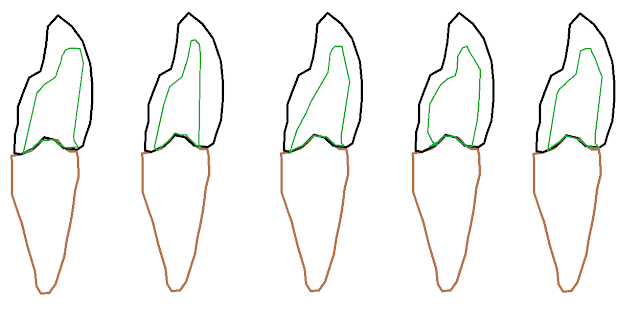
Anterior tooth forms are simple to design when broken down into parts. As covered in previous blog posts we start the design with a rectangle. The length of the tooth is determined when considering the incisal edge and gingival margin positions. From this, the mesial-distal dimension can be judged when considering the ideal ratio of the tooth as it sits in the mouth. Once the position and size of the central incisor is defined, the other teeth can be designed more posteriorly. Canines are narrower than canines anatomically but tend to be the same length. Therefore then appear thinner in proportion. The rectangle defines the border of the tooth as viewed from the labial. From here, defining certain points on the borders of the rectangle will allow you to join the dots and define the form of the tooth (Figure1) . These points are: -Mesial and distal contact points which also define the incisal embrasures (the negative space that is formed between the incisal edge and interproximal sur...