Skip to main content
Analysing the aetiology of tooth wear
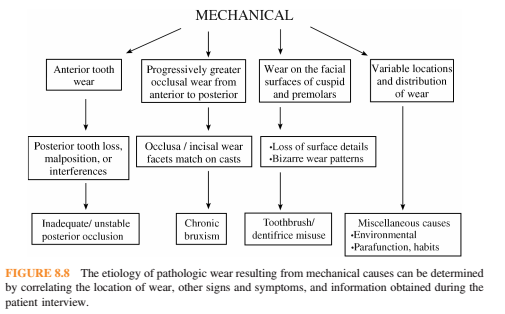
- Mechanical wear: Restorations tend to wear at the same rate as surrounding tooth structure. Displays sharply defined peripheries that can be matched on articulated diagnostic casts. Frequently asymptomatic and patients may report parafunctional habits
- Anterior wear greater than posterior wear: Posterior tooth loss, malposition or interferences
- Inadequate or unstable posterior contacts-> anterior teeth taking more force-> anterior wear and loss of vertical dimension
- Posterior occlusal premature contacts-> anterior posturing-> increased function-> wear
- Progressively greater wear on the anterior teeth: (Exception in anterior open bite). Bruxism. May also show grooving of the lateral borders of the tongue, evidence of cheek biting, fracture of porcelain restorations. Cupping or cratering of the occlusal surfaces can occur once the enamel has been perforated.
- Facial surface of canines and premolars: Excessive toothbrushing resulting in a sandblasted appearnce with a loss of anatomic detail. Ask the patient to demonstrate their brushing technique to see if it correlates with wear areas.
- Wear in variable locations primarily occlusal and incisal: Some form of parafunctional habit which may be job related e.g pipes, pins, needles, paper clips, sunflower seeds, soft drink cans.
- Diagnostic algorithm for mechanical wear:
- Determine character of wear
- Determine location
- Evaluate clinical signs and symptoms
- Chemical wear: Restorations appear elevated-> restoration islands. Occlusal surfaces display cupping and cratering with rounded margins. Frequently hypersensitive and not stained. Wear cannot be matched on opposing diagnostic casts. Occurs in stages: Smoothly glazed enamel which progresses to concavities then islands of restorations which lead to cupping
- Anterior surface loss greater than posterior surface: Progressively greater erosive damage from posterior to anterior.
- Palatal surface of the upper teeth-> Chronic vomitting, hiatal hernia, gastric reflux. Palatal surfaces are very smooth. Maxillary molars and premolars have chamfer like margins on the palatal surfaces.
- Gastric reflux has less volume of vomitus and no forceful expulsion due to no contraction of the diaphragm. GERD is suggested by belching, acidic taste in the mouth, stomach aches on awakening, heartburn, hypersensitivity of the affected teeth but many patients can be asymptomatic and pH monitoring may be needed.
- Chronic alcoholism-> gastritis-> chronic vomitting
- Facial surfaces of the maxillary anterior teeth and unaffected posterior teeth: Citrus fruit sucking
- Posterior surface loss greater than anterior surface loss: Acidic foods and drinks
- Erosion greatest at the mandibular 5 and 6: holding soft drink in mouth and swishing. Buccal mucosa and lateral tongue limit the effects to the occlusal surfaces resulting in restoration islands. Maxillary and mandibular anterior teeth are usually not affected
- Erosion evenly over occlusal surfaces of upper and lower indicates chewing of citrus fruits pulps. Increased in health conscious people e.g vegetarians.
- Variable locations: Miscellaneous causes
- Chewable vitamin C tablets, chewable aspirin tablets, aspirin powders
- Amphetamine, ecstasy wear of posterior occlusal surfaces
- Cocaine to the oral mucosa causes cervical erosion of the maxillary anterior and first premolar teeth
- Xerostomia
- Factory workers: Acidic aerosols
- Erosion on the facial surfaces of the anteriors: Professional wine tasters and swimmers



Comments
Post a Comment
Please leave a comment and let me know what you think or if there are any topics you would like covered in the future